PE 307: Kinesiology Notes
Muscle Fibers
Two major types of muscle shape fiber arrangements
Parallel | Pennate | |
|---|---|---|
Fiber arrangement description | Run parallel to length of muscle, have longer fibers | Run obliquely to tendons, have shorter fibers |
Range of motion (large or small) | large | |
C/S area | small | |
Strength/Power | small | |
Types | Flat: thin and broad, may run from aponeurosis. Fusiform: spindle shaped Strap: long fibers Radiate: triangular shaped (flat and fusiform combo) | Unipennate: fibers run from tendon on one side Bipennate: fibers run from both sides of central tendon Multipennate: fibers run from several tendons |
Four properties related to a muscle’s ability to produce a force:
Irritability | Being responsive to chemical, mechanical, or electrical stimuli |
Contractility | Ability to contract and develop tension or force when stimulated |
Elasticity | Ability to return to its original length following stretching |
Extensibility | To be stretched back to its original length following contraction |
Intrinsic muscles are located within the body part on which they act. Ex: hand, foot
Extrinsic muscles are located outside the body part on which they act.
The origin is the proximal attachment, considered the least movable part and attaches closest to the midline.
The insertion is the distal attachment, considered the most movable part.
Two types of muscle action:
1. Isometric/Static: tension develops within the muscle, but the joint angle remains constant.
2. Isotonic/Dynamic: Tension develops within the muscle to cause or control joint movement.
Two types of isotonic:
1. Concentric: muscle develops tension as it shortens, force developed is greater than the resistance, “speeds up” resistance, joint angle changes in the direction of the applied muscular force.
2. Eccentric: muscle develops tension as it lengthens, force developed is less than the resistance. Keeps the weibght/resistance from being accelerated downwards by gravitational force in traditional weight training exercises.
N.B. Movement may occur at any given joint without muscle contraction, this is referred to as a passive (as opposed to active) movement due to the external force(s) (e.g. gravity, resistance, relaxation, therapist moving joint through its range of motion)
Careful of the etymology. Iso = same, tonic = tension (“isokinetic” is a form of rehab. Ex cybex or biodex)
Role of Muscles
- Agonists/prime movers: primary muscles that initiate and carry out the action
- Antagonists: muscles that oppose the action of the agonist muscles. Usually located on the opposite side of the joint from the agonist, they work in cooperation with the agonist by relaxing and allowing movement.
- Stabilizers: muscles that surround the joint or body part and contract to stabilize the area to enable another limb to exert force and move
- Synergist: assist in the action of the agonist
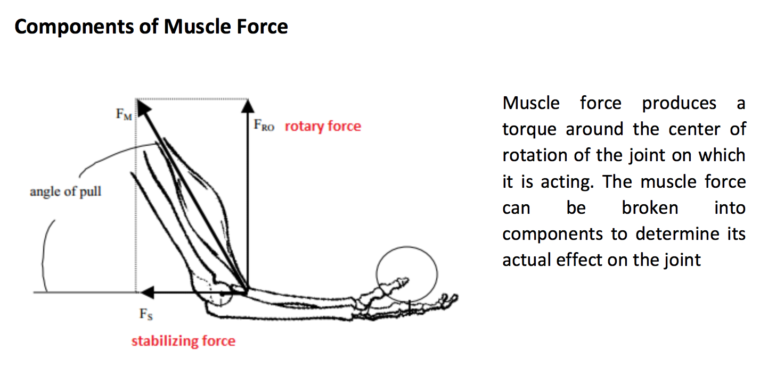
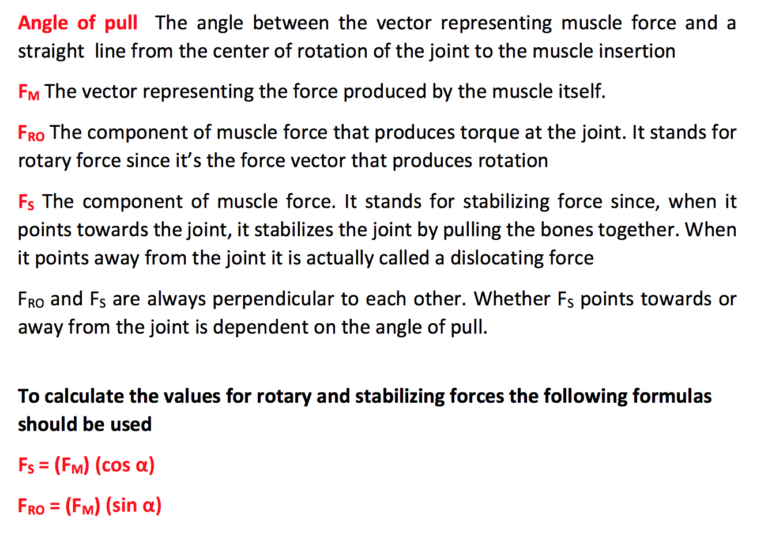
- Line of pull: the resultant force produced at an attachment by a muscle.
- Angle of pull: the angle between the ‘line of pull’ of the muscle and the bone on which it inserts
Neuromuscular Concepts
All or none principle: When a motor fiber is stimulated, all of the muscle fibers in that motor unit contract to their fullest extent or they do not contract at all.
Muscle length-tension relationship: the maximal ability of a muscle to develop tension/force varies, depending on the length of the muscle during contraction. Generally, a muscle can develop the greatest amount of force/tension if it’s stretched 100-130% of its resting length.
Muscle force-velocity relationship: as the force needed to cause movement of an objects increases, the velocity of concentric action decreases, whereas the velocity of eccentric action increases (at least until the point at which control is lost)
Biarticular muscles: cross and act on two different joints
Multiarticular muscles: Cross and act on 3+ joints
Reciprocal inhibition/innervation: Neuromuscular phenomenon in which the innervation, contraction/shortening of agonist muscles is accompanied by the inhibition of the antagonist muscles.
Active and passive insufficiency: as a muscle shortens, its ability to exert force diminishes. When a muscle becomes shortened to the point it cannot generate or maintain active tension, active insufficiency is reached. If the opposing muscle becomes stretched to the point where it can no longer lengthen and allow movement, then passive insufficiency is reached.
Misc.
Goniometer: a device used in OT, PT, AT, etc that measures joint angle and ROM